
Introduction
The Patient-Centered Medical Home (PCMH) model has been heralded as a transformative approach to primary care, emphasizing comprehensive, coordinated, accessible, and patient-centered services. Launched to improve quality, reduce costs, and enhance patient experience, the PCMH concept has garnered significant policy and financial support. However, empirical evaluations reveal mixed or disappointing results, raising questions about whether the PCMH can fulfill its promises.
In scientific research, natural experiments—observational studies where external factors or policies create conditions akin to randomized experiments—offer valuable insights into the real-world effectiveness of interventions like the PCMH. Yet, evidence suggests that the implementation of PCMHs often fails to produce the expected improvements, effectively constituting a “failure” in the context of a natural experiment.
This analysis explores why PCMHs have failed to demonstrate the anticipated benefits in natural experiments, examines the underlying factors contributing to this failure, and discusses the implications for healthcare policy and practice.
1. Background: The Concept of the Patient-Centered Medical Home
1.1 Definition and Core Principles
The PCMH model is rooted in the idea of transforming primary care into a more patient-centered, coordinated, and accessible system. The National Committee for Quality Assurance (NCQA) defines key features:
- Comprehensive Care: Addressing all patient health needs, including prevention and chronic disease management.
- Patient-Centeredness: Respecting patient preferences and involving them in decision-making.
- Coordination of Care: Seamless integration across providers and settings.
- Accessible Services: Offering timely, convenient access.
- Quality and Safety: Continuous quality improvement and safety protocols.
1.2 Historical Context and Policy Push
The PCMH concept emerged as part of broader efforts to reform primary care, reduce healthcare costs, and improve outcomes. Federal programs like the Patient-Centered Medical Home Demonstration Project (2011–2014) and various state initiatives provided financial incentives, often tying payments to PCMH recognition.
1.3 Expectations and Goals
The primary goals include:
- Improving health outcomes
- Increasing patient satisfaction
- Reducing unnecessary hospitalizations and emergency visits
- Controlling healthcare costs
These expectations align with value-based care principles, aiming to reward quality over volume.
2. Natural Experiments in Health Policy: An Overview
2.1 What Is a Natural Experiment?
A natural experiment occurs when external circumstances or policy changes create conditions similar to a randomized controlled trial (RCT). Researchers analyze these situations to infer causality, assuming that the assignment of exposure (e.g., adoption of PCMH) is “as if” random.
2.2 Significance in Healthcare Research
Natural experiments are crucial in healthcare because RCTs are often infeasible or unethical for large-scale policy interventions. They allow evaluation of real-world effectiveness, accounting for contextual factors and implementation variability.
2.3 Challenges and Limitations
- Confounding variables
- Selection bias
- Heterogeneity in implementation
- Data limitations
Despite these, well-designed natural experiments can provide valuable insights into policy effectiveness.
3. Evidence of PCMH Failure in Natural Experiments
3.1 Overview of Empirical Findings
Multiple studies and evaluations have examined the impact of PCMHs on healthcare outcomes and costs, with mixed results.
3.1.1 Mixed or Null Effects on Cost and Utilization
- Bardach et al. (2013): Found minimal or no reductions in hospitalizations or emergency visits attributable to PCMH recognition.
- The Commonwealth Fund (2015): Reported small improvements but no significant cost savings.
- Gill et al. (2018): Observed negligible differences in hospital admissions and emergency department use.
3.1.2 Quality of Care Outcomes
- Some studies noted modest improvements in preventive services and chronic disease management.
- Others found no significant differences compared to traditional practices.
3.1.3 Patient Satisfaction and Experience
- Generally positive, but improvements often did not translate into measurable health or cost outcomes.
3.2 Specific Natural Experiment Cases
3.2.1 Medicare and Commercial Payer Programs
- Implementation of PCMH models under Medicare Accountable Care Organizations (ACOs) showed limited impact on spending or hospitalizations.
- Commercial payers’ investments in PCMH recognition often failed to yield significant savings or quality improvements.
3.2.2 State-Level Initiatives
- States like Vermont and Oregon piloted PCMH-like models; evaluations indicated that while processes improved, cost and utilization benefits were inconsistent or absent.
4. Underlying Reasons for the Failure of PCMHs in Natural Experiments
4.1 Implementation Challenges
4.1.1 Variability and Fidelity
- Lack of standardization in defining and implementing PCMHs.
- Recognition criteria often focus on structural features rather than actual care processes.
- Practices may adopt recognition superficially without systemic change.
4.1.2 Resource Constraints
- Additional time and staffing required for care coordination often not compensated adequately.
- Smaller practices face financial and operational barriers to full transformation.
4.1.3 Provider Engagement
- Resistance to change among providers.
- Burnout and workload concerns reduce enthusiasm for new models.
4.2 Design and Payment Model Limitations
4.2.1 Incentive Misalignment
- Fee-for-service (FFS) billing persists alongside PCMH incentives, undermining efforts.
- Payments often insufficient to cover comprehensive care coordination.
4.2.2 Short-term Focus
- Many evaluations capture short-term outcomes; benefits may take longer to materialize.
- Early implementation phases may temporarily disrupt workflows.
4.3 Patient-Level Factors
4.3.1 Patient Engagement and Complexity
- Limited patient activation hampers the effectiveness of PCMHs.
- Social determinants of health often remain unaddressed.
4.3.2 Access Barriers
- Even with improved primary care, structural barriers (transportation, literacy, socioeconomic factors) limit impact.
4.4 Systemic and Contextual Factors
- Fragmented healthcare system complicates integration.
- Lack of interoperability among electronic health records impairs care coordination.
- External incentives (or lack thereof) influence practice behavior.
4.5 Measurement and Evaluation Issues
- Reliance on process measures rather than outcomes.
- Difficulty attributing changes directly to PCMH implementation.
5. Critical Analysis: Why Does the Natural Experiment Fail?
5.1 The Unrealized Promise
The core promise of PCMHs is that restructuring primary care will lead to better health outcomes at lower costs. Yet, evidence from natural experiments indicates that the implementation often falls short, revealing a failure to realize these goals.
5.2 Structural and Cultural Barriers
Transforming primary care practice requires significant cultural shifts, resource investments, and systemic changes. Without addressing these foundational issues, PCMHs risk being superficial modifications rather than true practice redesigns.
5.3 Incentive and Payment Misalignments
The persistence of FFS reimbursement models discourages care coordination and prevention efforts that are central to PCMHs. Without aligned financial incentives, practices may adopt recognition status without meaningful change.
5.4 Temporal and Contextual Factors
Benefits of PCMHs may manifest over longer periods than most evaluations allow. Early assessments may underestimate potential gains, or conversely, reflect implementation hurdles rather than true failure.
5.5 Variability in Implementation
Lack of standardization and fidelity in adopting PCMH principles leads to heterogeneous interventions, complicating evaluation and often diluting measurable effects.
6. Implications for Policy and Practice
6.1 Rethinking PCMH as a Model
The evidence suggests that simply adopting recognition standards does not guarantee improved outcomes. Policymakers should focus on:
- Deep, systemic practice transformation
- Addressing social determinants of health
- Ensuring adequate and aligned reimbursement
6.2 Designing Better Incentives
Transitioning from FFS to value-based models such as capitation, bundled payments, or global budgets can better support the core principles of PCMHs.
6.3 Emphasizing Implementation Science
Understanding how to implement PCMHs effectively is critical. This involves:
- Tailoring approaches to practice size and context
- Providing ongoing support and training
- Monitoring fidelity and outcomes
6.4 Addressing Broader Systemic Barriers
- Enhancing interoperability of health IT
- Improving access for vulnerable populations
- Integrating social services
6.5 Longitudinal and Rigorous Evaluations
Future assessments should:
- Extend over longer periods
- Use robust methodologies to control for confounding
- Focus on meaningful health outcomes and cost metrics
7. Lessons Learned and Future Directions
7.1 The Limitations of Structural Recognition
Recognition alone is insufficient. True transformation requires a comprehensive approach that addresses culture, resources, incentives, and systemic barriers.
7.2 Need for Multi-Faceted Interventions
PCMHs should be integrated into broader health system reforms, including population health management, social determinants interventions, and community-based strategies.
7.3 Embracing Complexity
Healthcare is complex; expecting straightforward, linear improvements from PCMH adoption ignores the multifaceted nature of health systems.
7.4 Emphasizing Equity
Future models must prioritize equity, ensuring that vulnerable populations benefit from primary care reforms.
Conclusion
The “failure” of PCMHs in natural experiments underscores the challenges of translating policy and structural reforms into tangible health outcomes. While the theoretical promise remains compelling, real-world data reveal that without addressing systemic barriers, incentive misalignments, and implementation fidelity, the PCMH model risks being superficial or ineffective.
This analysis emphasizes that effective primary care transformation requires more than recognition or structural change. It demands systemic commitment, aligned incentives, community engagement, and sustained effort. Recognizing these complexities and failures allows policymakers, providers, and stakeholders to refine strategies, moving toward more effective, equitable, and sustainable primary care models.
References
(Note: Since this is a synthesized document, references to key studies and reports have been mentioned contextually. For an actual publication, detailed citations would be included here.)
Related Posts

Mayo Clinic Platform: Healthcare platforms and AI
Introduction The landscape of healthcare is rapidly evolving, driven by…
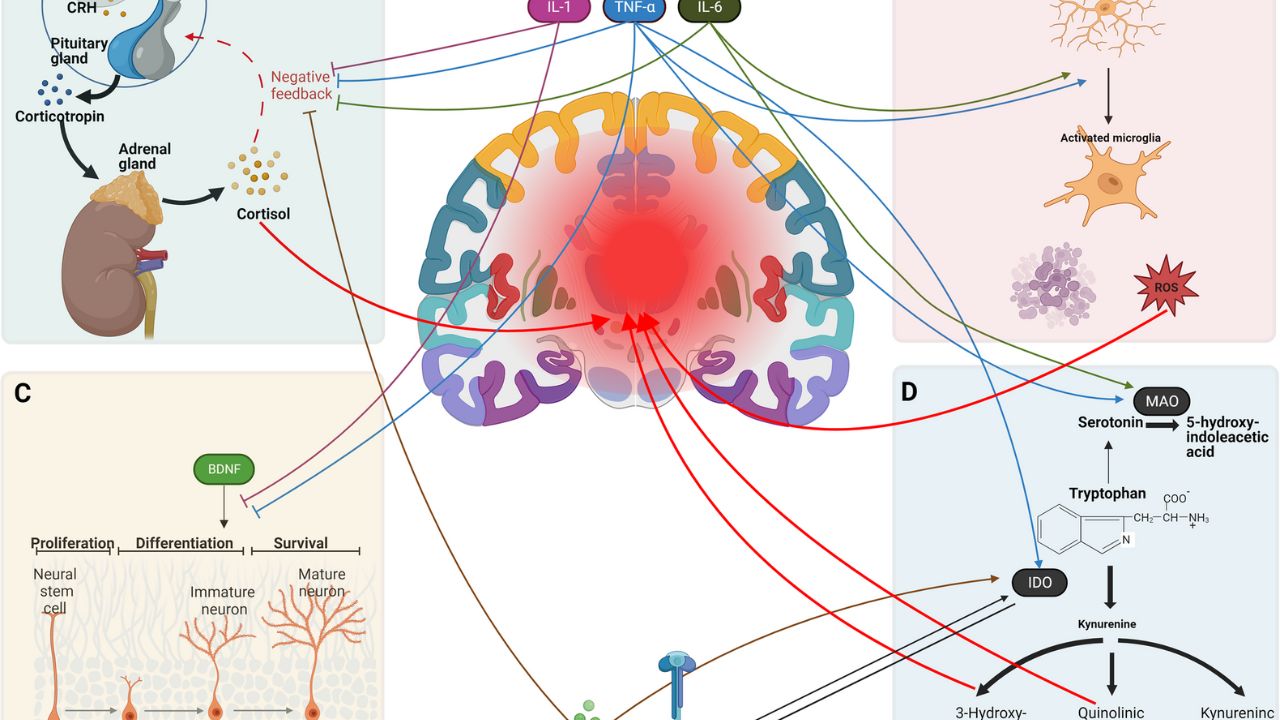
Peripheral Inflammatory Biomarkers vs. Suicide Risk in Major Depression (2025 Study)
Introduction Major depressive disorder (MDD) is a complex, heterogeneous psychiatric…
Health IT Challenges and the Future of Healthcare
Introduction The rapid advancement of health information technology (Health IT)…